
American medicine did not accidentally drift into its current imbalance between cognitive and procedural care. It was built that way, step by step, over the past 75 years.
The American Medical Association played a central role, not as the sole actor, but as the architect of key structures that continue to shape how physicians are paid and how care is valued.
Core Problem
The core problem is simple: our system pays more for doing than for thinking.
In the decades following World War II, the AMA successfully opposed national health insurance and supported a private, insurance-based model. That decision had long-term consequences.
Private Insurance
Private insurance evolved around itemized billing for discrete services. Procedures fit neatly into that framework. Cognitive care does not. Managing complex patients, synthesizing data, coordinating care, and making nuanced clinical decisions are harder to define, measure, and price.
Current Procedural Terminology System
The next pivotal step came in 1966 with the creation of the Current Procedural Terminology, or CPT. This coding system, developed and maintained by the AMA, became the language of American medicine. It standardized how services were described and billed.
CPT grew in a procedural world. Procedures were easier to specify, defend, and monetize. Cognitive services, by contrast, were compressed into time-based visit codes that never fully captured complexity or intensity.
Resource-Based Relative Value Scale
The modern payment structure was cemented in 1992 with the adoption of the Resource-Based Relative Value Scale. This system assigns relative value units, or RVUs, to physician services.
In theory, RVUs account for time, intensity, and practice expense. In practice, they rely heavily on recommendations from the AMA-convened Relative Value Scale Update Committee, known as the RUC.
Relative Value Scale Update Committee
The RUC became the quiet center of gravity in physician payment. Specialty societies generate the data. They survey their members. They recommend values. Procedural specialties, with more discrete and measurable work, have been well positioned in this process. Cognitive specialties have not.
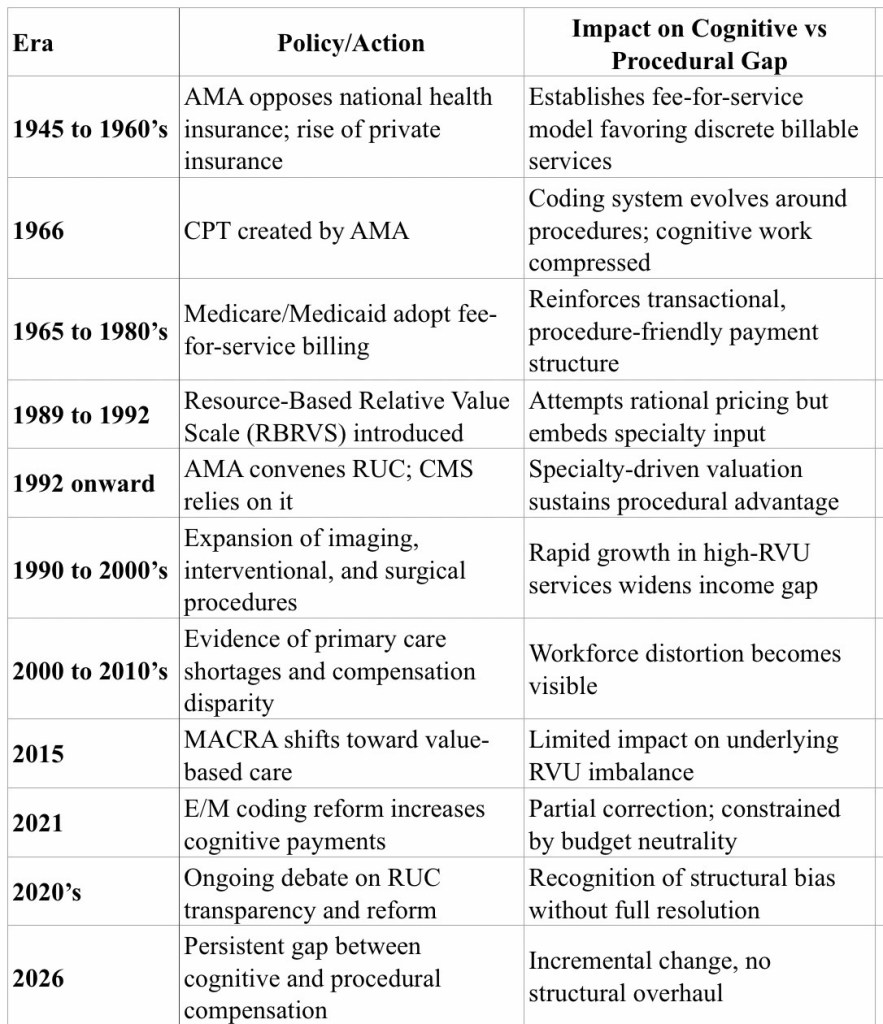
Key Payment Policy Moments (1945–2026)
The result was predictable.
Procedures retained high valuations, often based on legacy assumptions about time and intensity. Cognitive care remained undervalued, even as patient complexity increased. Over time, this created a widening gap in compensation, influence, and workforce distribution.
Three structural features reinforced the imbalance.
First, procedures are inherently easier to quantify. A surgery has a defined start and end. Cognitive care unfolds over time, often invisibly. Much of its value lies in what does not happen, avoided complications, unnecessary admissions, fragmented care.
Second, the valuation process relies on survey data that tends to reflect the interests of those generating it. Once a procedure is highly valued, it is difficult to recalibrate downward. Cognitive services, lacking similar advocacy strength, lag behind.
Third, Medicare’s budget neutrality requirement turns reform into redistribution. When cognitive codes are increased, procedural payments are often cut. This creates resistance and slows meaningful change.
Governance matters as well.
The AMA House of Delegates and associated committees include broad representation, but specialty societies have substantial influence. The same organizations that benefit from higher procedural valuations are embedded in the structures that maintain them.
To be clear, this was not the result of malicious intent. It was the cumulative effect of incentives, structure, and representation. But the outcome is unmistakable: a system that undervalues the work of managing complexity, building relationships, and thinking through uncertainty.
Correction Attempts
There have been attempts at correction. The 2021 revisions to evaluation and management coding modestly increased payment for cognitive care and reduced documentation burden. These were meaningful, incremental improvements. And they did not fundamentally rebalance the system.
Consequences
The consequences extend beyond physician compensation. They shape career choice, contributing to shortages in primary care and cognitive specialties. They influence practice models, pushing physicians toward volume and procedures. They affect patient care, particularly for those with chronic, complex conditions who rely on longitudinal management.
The Future?
If we want a healthcare system that rewards value rather than volume, we need to address the architecture itself.
That means rethinking how we define and measure cognitive work. It means reforming the valuation process to reduce specialty-driven bias. It means reconsidering budget neutrality when it prevents necessary investment in underpaid areas of care.
Most importantly, it means recognizing that the hardest work in medicine is often not procedural. It is cognitive. It is longitudinal. It is invisible.
Until we value that work appropriately, the imbalance will persist.
Future article: How does artificial intelligence and private equity fit in with this unique American healthcare system? 

Interesting. Although slightly different in context, this resonates with my experience of having a subarachnoid hemorrhage from a bicycling accident. An invisible and very complex injury that no procedure was going to fix.
LikeLike